A Statistical Analysis of Medical Facilities in Satara District: Geographical Study
Yadav SS1*, Wagh AS2, Nimbale SM3
DOI:10.5281/zenodo.16750405
1* Sushil S. Yadav, Research Scholar, Department of Geography, Shivaji University, Kolhapur, Maharashtra, India.
2 Arjun Shivaji Wagh, Assistant Professor, Padmabhushan Dr. Vasantraodada Patil Mahavidyalaya, Tasgaon, Sangali, Maharashtra, India.
3 Sharadkumar M. Nimbale, Assistant Professor, Yashavantrao Chavan Institute of Science, Satara, Maharashtra, India.
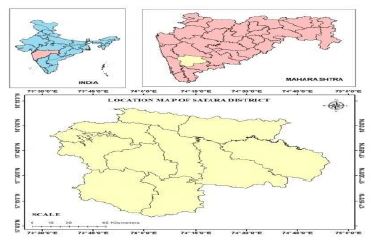
This study presents a comprehensive statistical analysis of medical facilities provided by Government in Satara district, aiming to provide insights into the healthcare infrastructure and accessibility in the geographical region. The Satara district is a located in the state of Maharashtra, India, encompasses diverse geographical and demographic characteristics, making it imperative to understand the distribution and adequacy of medical resources. Key Statistical Indicators such as the number of healthcare facilities per capita, bed capacity, availability of medical staff, and infrastructure are analyzed to assess the overall healthcare provision in Satara district. Moreover, the study evaluates the geographical distribution of medical facilities to identify potential gaps and disparities in healthcare access, particularly in rural and remote areas. The findings of this study contribute valuable insights for healthcare policymakers, practitioners, and stakeholders to formulate targeted interventions and policies aimed at enhancing the quality and accessibility of healthcare services in Satara district. By addressing the identified gaps and leveraging existing resources effectively, it is envisaged that the overall health outcomes and well-being of the population in Satara district can be significantly improved. It will be fide out the role of medical facilities in human development index.
Keywords: statistical analysis, health index, population, demographic characteristics, accessibility
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Research Scholar, Department of Geography, Shivaji University, Kolhapur, Maharashtra, India. Email:  |
Yadav SS, Wagh AS, Nimbale SM, A Statistical Analysis of Medical Facilities in Satara District: Geographical Study. Soc Sci J Adv Res. 2025;5(4):90-97. Available From https://ssjar.singhpublication.com/index.php/ojs/article/view/271 |
 |
 ©
©